Thursday, September 29
ACUTE BRONCHOPNEUMONIA
Reader Cris (are you my high-school classmate, by any chance?) asks about acute bronchopneumonia in my tagboard over at PARALLEL UNIVERSES. He says his son has just been diagnosed with the ailment, and I think he's quite worried.
Let us first know what acute means, and how to differentiate it with chronic. Acute is anything that happens abruptly as contrasted with chronic, which may be long-standing.
In the case of Cris' son, the diagnosis of acute bronchopneumonia means that the doctor has concluded that there was no respiratory illness of the same character in the child, say, a week or days before the consult.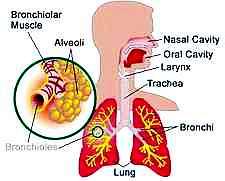 Why was the diagnosis not simply termed as "pneumonia," as we are all most familiar with? Why the prefix "broncho-?"
Why was the diagnosis not simply termed as "pneumonia," as we are all most familiar with? Why the prefix "broncho-?"
The prefix "broncho-" means that the doctor who made the diagnosis is quite sure that the pneumonia affecting the child is confined to the bronchiolar part of the lungs.
As with all other pneumonias, this illness is best described as inflammation of lung tissue, and manifests itself as cough, and notable fast and difficult breathing. The leading culprits are Streptococcus pneumoniae and Haemophilus Influenzae. Respiratory viruses like influenza, parainfluenza, RSV, and adenoviruses are likewise implicated, but they seldom cause fatal infection than their bacterial buddies. The best way to identify is to request a laboratory culture of the organism.
Pneumonia affects an estimated 5 to 10 percent of all children less than 5 years old, especially those living in developing countries like the Philippines. It is transmitted through person-to-person contact, and usually after touching or inhaling infected secretions.
Treatment is by the use of antibiotics or anti-retroviral medications. Prevention is still the best cure. This is achieved by proper hygienic practices, isolation of infected patients, and vaccination. Conjugate vaccines are available for H. influenza type B and S. pneumonia.
More information on this link: Bronchopneumonia and
See How the Lung with Bronchopneumonia Looks Like
Dr. Emer at 4:46 PM

Tuesday, September 14
CHELATION THERAPY FOR CORONARY ARTERY DISEASE
My friend and loyal reader Bayi requested this post which I'm sure others will also find useful.
A quick answer to the question whether chelation therapy works for coronary artery disease or CAD cannot be readily given because the medical community both here and abroad is still split on the true answer. Some will say yes. Most will say no. Chelation therapy falls under the category of "alternative treatment modalities" which patients seek after all conventional medical treatment options have failed them.
Chelation therapy is approved by the US FDA for treatment of heavy metal poisoning. In spite of its reported benefits for coronary artery disease which are largely anecdotal in nature, it has NOT been approved by any health regulating agency as treatment for CAD. 
Chelation therapy involves the intravenous infusion of EDTA or ethylenediamine-tetraacetic acid into the body of a patient wishing to have the therapy. EDTA has a very high affinity and can indiscriminately bind minerals and heavy metals like aluminum, arsenic, cadmium, calcium, copper, iron, lead, nickel, and mercury. This particular ability to bind heavy metals explains why it is useful in cases of heavy metal poisoning.
How then did it become famous as an alternative treatment for coronary disease?
Let's have a little history lesson: "Administration of chelation therapy expanded to other conditions, such as heart disease, in the 1950s. While treating workers in the battery industry for lead accumulation, Norman Clarke, Sr., MD, noticed that some patients had improved (from their) angina (conditions) after chelation therapy.
In CAD, the coronary arteries or the blood vessels of the heart develop fatty deposits along its luminae (called plaque) and over time, cause a blockade of the affected vessels. When the block becomes severe, say, 80 percent or more --- which can be seen in an angiogram --- oxygen-rich blood which the heart needs can't get through and this is when the symptoms of heart attack set in: one feels chest pains (angina) and shortness of breath (dyspnea).
"In theory, progression of atherosclerosis depended on copper, iron, or other minerals, such as calcium, and chelation therapy could bind these minerals and inhibit the process. Chelation therapy for patients with heart disease fell out of favor in the 1960s.
"In 1972, the remaining proponents of chelation therapy founded the American College for the Advancement of Medicine to promote and perform research on chelation therapy.
"Today, more than 1000 physicians practice chelation therapy in the United States. However, whether the potential benefits of this therapy outweigh the risks still remains highly controversial." [Pharmacotherapy 22(8):1067-1069, ©2002 Pharmacotherapy Publications thru Medscape.com]
There are doctors who say that the primary theory in which chelation therapy is based, does NOT make sense at all.
Among them is clinical cardiologist John Barnard, from St. Luke's-Roosevelt Hospital in New York City, who calls chelation therapy "a worthless therapy that is expensive and time-consuming." He further explains his point: "The more calcium that is in the arteries, or the higher the calcium score, the more likely and the more severe the coronary artery disease is, so the (chelation therapy) theory always was if you get rid of the calcium then, that should fix the arteries and the arteries should improve.
In the US, a single chelation treatment takes about 2 hours and typically costs anywhere from $75 to $110. This is 2001 data and prices may have gone up by this time. Oftentimes, 25 to 40 treatments are required. And since it is an alternative form of treatment, medical insurance does not cover it, so it is usually patients who must foot the bills. [AP report ©2001]
"(But) the problem is calcium buildup forms later (and) AFTER cholesterol (deposition) so once the arteries are calcified, the damage is already done." [News8 Austin]
Are there any risks or side effects to chelation therapy?
I've taken the answer straight from the TACT webpage: "Chelation with EDTA has been used to treat heavy metal poisoning such as lead. For this use, there is a low occurrence of side effects. The safety of EDTA for treating heart disease has not been established.
There you have it, Bayi.
"The most common side effect is a burning sensation at the site where the EDTA is delivered into the vein. Rare side effects can include fever, headache, nausea, and vomiting. Even more rare are serious side effects that can include a sudden drop in blood pressure, abnormally low calcium levels in the blood, permanent kidney damage, and bone marrow depression (meaning that blood cell counts fall). Reversible injury to the kidneys, although infrequent, has been reported with EDTA chelation therapy. Other serious side effects can occur if EDTA is not administered by a trained health professional.
"In addition, because chelation therapy removes important vitamins and minerals from the body, it will be very important for you to take the vitamin supplements supplied by the study. It is also important that you continue to take your standard heart disease treatments." [Chelation Therapy Study]
I still will not recommend chelation therapy for coronary heart disease.
And for those who might want additional medical opinions on other "alternative" treatment options for cardiovascular diseases like garlic, fish oil, vitamin E, soy protein, coenzyme Q10, gugulipid and hawthorne, I invite you to read this insightful article from the 37th Annual American Society of Health System Pharmacists Midyear Clinical Meeting held from December 8 to 12, 2002, in Atlanta, Georgia. It might be 2 years old, but it is still very enlightening.
Dr. Emer at 10:40 PM
Wednesday, September 8
DISCLAIMER
The THIRD OPINION does not intend to replace your physician's medical evaluation of your condition. It merely presents an alternate opinion of the queries submitted. There may be cases when the opinion expressed is similar to what has already been given to you. When in doubt, you can have as many opinions from as many physicians as you want, but the final decision rests in your hands. You and you alone can decide what is best for yourself or your loved ones. This weblog only aims to help you make an informed decision.
There is a Chinese saying that goes:
"A wise man makes his own decisions, an ignorant man follows public opinion."Whatever you decide, be firm about it, be confident about it, and be happy about it.
God bless you.
Dr. Emer at 12:04 PM